CDC CARE (Check and Report Ebola) Hotline

After a rapid and agile development strategy, an Ebola-Monitoring IVR solution was piloted with Centers for Disease Control and Prevention (CDC) federal employees who returned from deployments to countries with Ebola outbreaks.

Platform Tools Used:


Location:

SUMMARY
The response to the 2014-2016 Ebola epidemic in West Africa included an unprecedented effort from federal, state, and local public health authorities to monitor all travelers entering the United States from countries with Ebola outbreaks for a period of 21 days after departure from the affected country. The Check and Report Ebola (CARE) Hotline, a novel approach to monitoring, was designed to allow travelers to report their health status daily to an interactive voice recognition system (IVR). After a rapid and agile development strategy, the IVR solution was piloted with Centers for Disease Control and Prevention (CDC) federal employees who returned from deployments to countries with Ebola outbreaks. The system was designed using open source tools from InSTEDD, Verboice for IVR, and mBuilder for short message service (SMS). These tools were packaged together and used to facilitate CDC employees’ adherence to daily reporting requirements.
CDC surveyed participating CDC employees to assess user experience. Results indicated that users became more familiar with and found the system easier to use over the course of their monitoring period. Most users were highly satisfied with the IVR system and would recommend it for future monitoring efforts. This technology is easily adaptable and can be modified for future emergency responses, contact investigations, or routine monitoring for public health protections.
IMPACT
Our pilot primarily sought to explore the following:
- To promote behavior change in the form of facilitating traveler adherence to post-arrival monitoring requirements for potential Ebola symptoms.
- To decrease the time to detection and time for response for potential cases of Ebola.
- To develop an adaptable reporting system that could be adjusted to a jurisdiction’s needs.
Results:
- We were able to quickly and easily design and deploy a robust reporting system.
- We were able to detect and follow-up with potential cases.
- We were able to document the costs associated with developing and implementing the IVR.
ADDITIONAL MEDIA
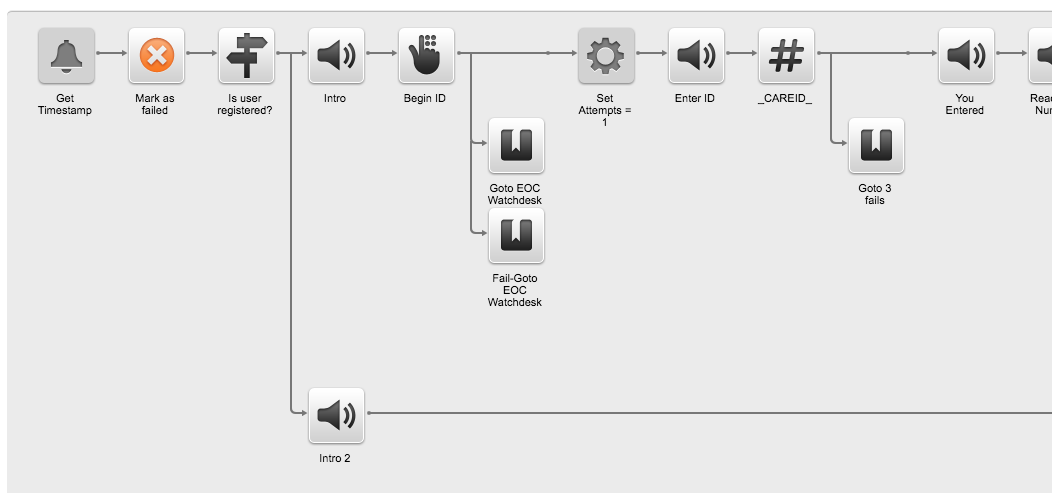
Call flow structure
A screenshot of a portion of the call flow structure for the CARE Hotline.
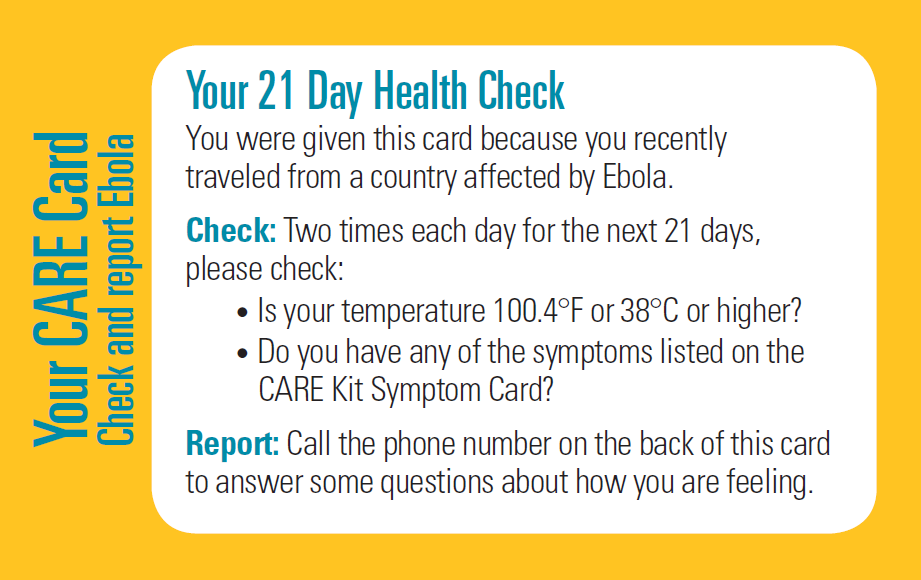
‘CARE Cards’
An early version of the CARE cards provided to travelers upon arrival to the United States from countries with Ebola Outbreaks. The CARE cards included instructions for conducting health checks and daily reporting.
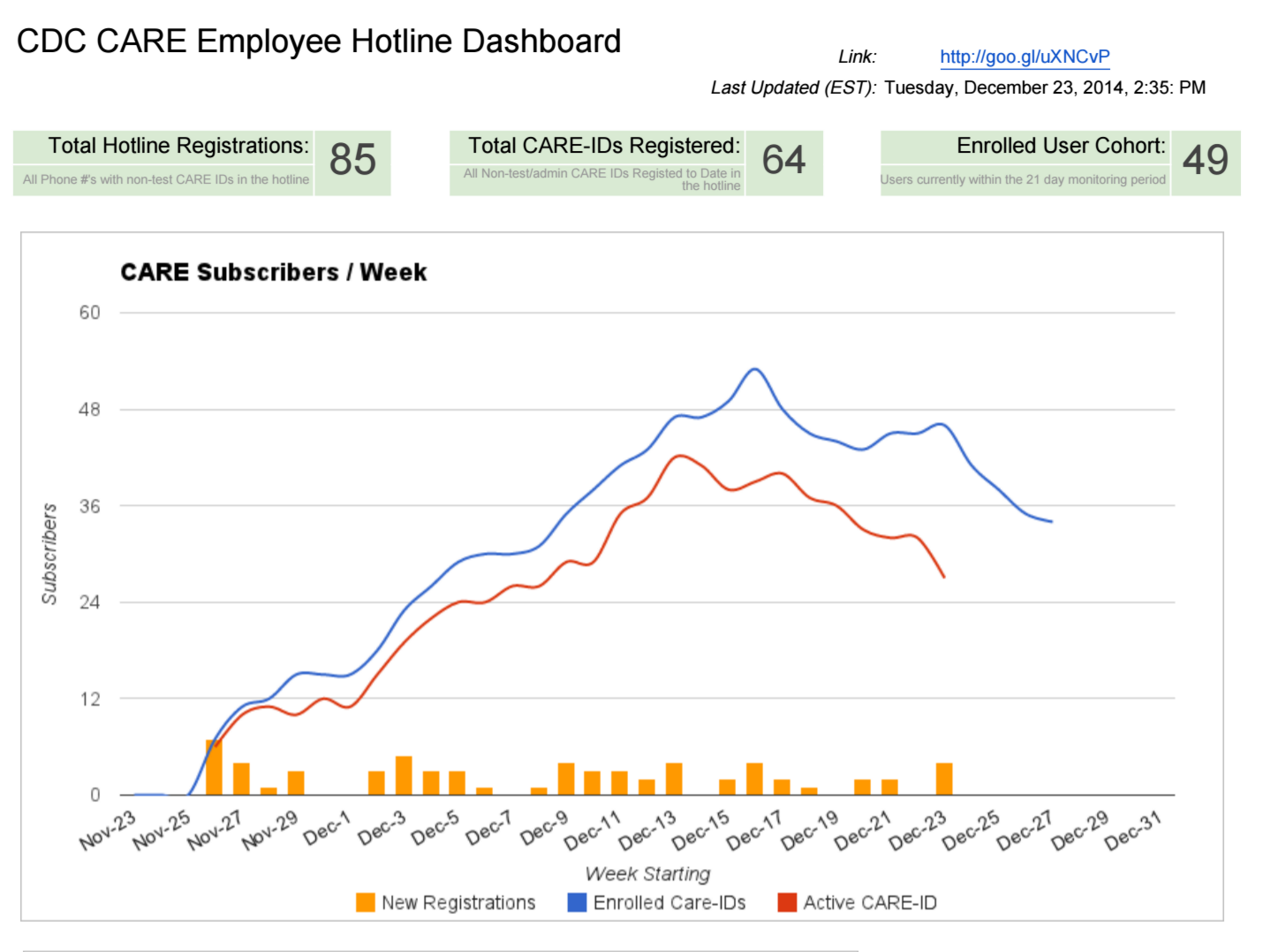
CARE Dashboard
A screenshot of the CARE Hotline dashboard. The first green box indicates the total number of unique phones numbers that accessed the hotline. Participants used multiple phone numbers (i.e. office phone, cell phone) to submit their health reports. The second green box indicates the number of CARE IDs registered with the hotline. Each traveler received a unique CARE ID number that they to register with the hotline. The third green box indicates the number of users enrolled in the system and within their 21 day monitoring period. The line graph the number of new registrations, enrolled users, and active users.
PROJECT CONTACTS
- From CDC DGMQ: Abbey Wojno (AWojno@cdc.gov); Heather Joseph (HJoseph1@cdc.gov)
- From InSTEDD: Scott Teesdale (steesdale@instedd.org)
Header graphic: UNMEER Flickr Thumbnail graphic: CDC Global Flickr